CHAPTER 6

Chewing and Sucking Lice
All lice are ectoparasites; that is, they live and
feed on the outside of their host's body. Although lice can have detrimental
effects on the host, an infestation is rarely, if ever, lethal. All
ectoparasites have a number of advantageous characteristics in common. Most are
quite small, flattened, wingless and possess
backward-projecting spines on their bodies. Their small size makes it more
difficult for the host to detect their presence. Being flattened and possessing
backward projecting spines that can lodge in hairs or feathers, these insects
are difficult to dislodge from the host. Finally, because the host represents
an unlimited source of food and typically is infested with many of these
ectoparasites, there is no need for wings to find food or a mate.
ORDER:
MALLOPHAGA (CHEWING LICE)
There are two orders of lice: namely the chewing lice
(Mallophaga) and the sucking lice (Anoplura). The orders can be separated by
the widths of their head. Chewing lice
mainly attack birds, although a few species inhabit mammals. They feed on hair,
skin debris, blood serum and secretions of the sebaceous glands. Eggs (nits)
typically are glued either to feathers or hair. The life cycle is generally
completed quite rapidly, with many species developing from egg to adult in as
little as 30 days. Chewing lice rarely leave the host and some have been
collected from museum specimens long after the death of the animal. All are
host specific with none living on humans. Heavy infestations of chewing lice on
poultry will result in loss of weight, reduced eggs production, and a general
rundown condition in an animal’s health.

A typical chewing louse with wide head and chewing type mouthparts.
Image courtesy of
Department of Parasitology,
ORDER: ANOPLURA (SUCKING LICE)
The sucking lice share the characteristics of all ectoparasites, but
differ from chewing lice by their mouthparts and width of their heads. The
chewing lice have large, heavily sclerotized chewing type mandibles for gnawing
on the host. Consequently, they possess large muscles to move the mandibles and
a large head that is needed to house the muscles. Sucking lice have small
needle-like mouthparts to suck the blood of their host and, correspondingly,
have smaller mouthpart muscles and a smaller head. With Mallophaga and
Anoplura, the head is wider and narrower than the thorax, respectively.
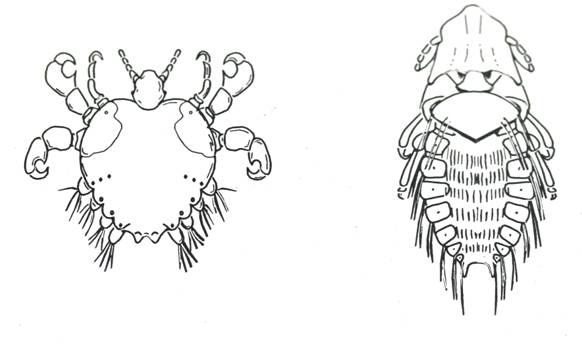
A comparison of width of head of a sucking louse and a sucking
louse.
Crab Lice. Sucking lice are chiefly found
on mammals. Almost all are host specific, with three types attacking humans:
namely the head, body and crab lice. Crab lice, Pthirus
pubis, also known as pubic lice, attack humans and a few species of
gorillas. The broad squat bodies, large claws on the middle and hind
legs, and characteristic sluggish movements have resulted in the pubic louse
aptly being called the crab louse. Infestations typically are restricted to the
groin and perianal area in adult humans; however, in very heavy infestations
they can be found all over the body. If a child who hasn't reached puberty is
attacked, the lice frequently are found on the eyelashes. Apparently this is because
one critical factor in crab louse environment is the distance between, and
thickness of, individual body hairs. This distance and coarseness in eyelashes
is ideal and consequently is occupied in the absence of pubic or other body
hair.
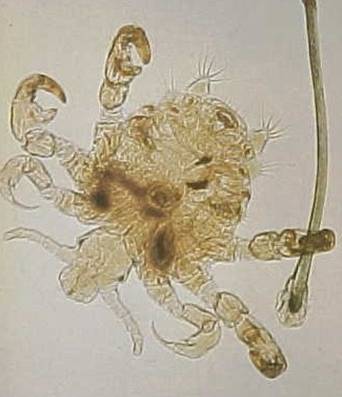
A crab louse. Image courtesy of
Females
lay a small number of eggs (100 to 150) on body hairs. Development is quite
rapid with the life cycle being completed in 30 to 40 days. Crab lice are
nearly immobile and typically attach to body hairs with their opposing claw-like
tarsi and tibia while feeding. They frequently become buried in their own
excrement and can only live for a short time off the host.
Because
of host dependency and relative immobility, these lice normally are acquired by
sleeping with an infested person. It is possible (but not probable), that crabs
could be contacted from situations such as using the same shower towel
immediately after an infested individual, using a toilet seat immediately after
use by a heavily infested individual or similar situations. As might be
expected, there is a correlation between the degree of crab louse infestation
in the general public in a given area or during a particular era and the degree
of sexual promiscuity. For example, crab lice infestations in the United States
during the 1960’s and 1970’s were more common than today. The 60’s and the 70’s
were the decades of social unrest, sexual experimentation and "free
love." Today, we are much more careful because our awareness of more
serious repercussions (AIDS, for example) has risen.
Crab lice do not vector any disease but
can cause a rash and corresponding itching. As do most blood sucking insects,
crabs inject a saliva when they feed that contains both an anticoagulant to
keep the host's blood flowing and an anesthetic to minimize detection of their
presence. Prolonged infestations of this species can result in subcutaneous
blue spots ranging in size from 1/16 to 1/2 inch in diameter. Of course, the
blue spots are a result of the anticoagulant in the saliva which results in
bruising.
There
are several products available for control of head lice. However, Kwell shampoo
is probably the most effective material available. It is formulated as a lotion
that contains the insecticide lindane. This insecticide has a relatively long
residual activity and readily penetrates the skin, qualities that are not found
in other products. Some doctors are not prescribing Kwell anymore because of
possible side effects. There are new medications being used recently that
approach Kwell in effectiveness but do not have the same side effects
Head Lice. Pediculus humanus capitis, and
body lice, Pediculus humanus humanus are different subspecies of the
same species. Placed side by side, they look almost exactly alike (Figure 6D);
however, they have quite different biologies and are easily distinguish from
crab lice (Figure 6E). It is thought that primitive humans were infested with
head lice but, as we became more civilized and began wearing clothing, this
opened up a different ecological niche that was occupied by body lice (body
lice are found on clothing). Because they are both the same species, they are
capable of inter-mating but their offspring all exhibit characteristics of head
lice.

A head or body louse with both appearing very
similar. Image courtesy of CDC.
Head Lice. Pediculus humanus capitis, and
body lice, Pediculus humanus humanus are different subspecies of the
same species. Placed side by side, they look almost exactly alike; however,
they have quite different biologies and are easily distinguish from crab lice.
It is thought that primitive humans were infested with head lice but, as we
became more civilized and began wearing clothing, this opened up a different
ecological niche that was occupied by body lice (body lice are found on
clothing). Because they are both the same species, they are capable of
inter-mating but their offspring all exhibit characteristics of head lice.
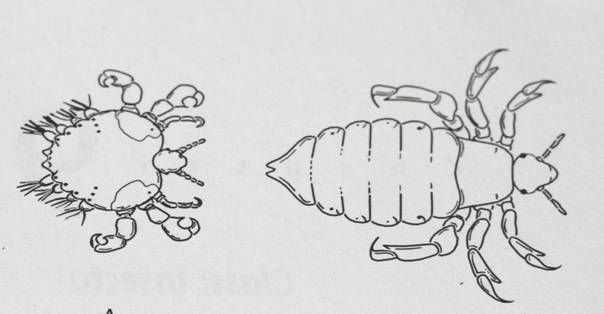
A head or body louse (right) compared to a crab louse (left).
Head lice were called mechanized dandruff during World
War II because typically they were found above the shoulders on scalp hair,
mustaches, sideburns and beards. Heavily infested individuals may have the lice
on all hairy parts of their bodies. They normally are gray colored, but tend to
take on the color of the hair they are infesting.

Relative Size of Head Lice Adults.
The eggs (nits) typically are deposited on the base of
the hair immediately next to the scalp. Generally, they hatch by the time the
hair has grown ¼ inch. Occasionally head lice will lay their eggs on long hair
that is lying on the scalp, so that unhatched eggs can be found some distance
from the base of the hair. Lice use cement that is impervious to normal
influences such as shampoo; consequently, the eggshells remain attached to the
hair long after hatching. Head lice are more prolific than crab lice because
the females can deposit up to 200 eggs and development can be completed in as
little as 30 days. It should be noted an infestation of head lice has no
correlation to unsanitary conditions and these lice have no socio-economic
barriers. The rich are as likely to be infested with these pests as are the
poor.

Nits on Human Hair.
There does seem
to be a correlation between the probability of being infested with head lice
and hair length. Probably this is due to the fact that these lice are more
difficult to control in longer hair. Also it is less common to find head louse
infestations in African-Americans: however, in Africa these lice readily attack
black individuals. lndividuals infested with these pests harbor only 10 to 20
lice, but in heavy infestations the hair can become matted with nits, nymphs
and adult lice. Typically, only the head or scalp of the host is infested, although the disease can occur in other hairy parts of the
body, like leg hairs. Head lice feed on human blood (hematophagy), and itching from louse bites is a common symptom of
this condition. Treatment
typically includes application of topical insecticides such as a pyrethrin or permethrin, although a variety of folk remedies are also common.

Head Louse Bite on Neck
Lice infestation in general is known as pediculosis, and occurs in many mammalian and bird
species. The term pediculosis
capitis, or simply "pediculosis", is sometimes used to refer to the
specific human pediculosis due to head-louse infestation. Humans are hosts for
two other lice as well—the body louse and the crab louse.
Head-louse infestations are widely endemic, especially
in children. It is a cause of some concern in public health, although, unlike
human body lice, head lice are not carriers of other infectious diseases. These infestations are most frequent on children
aged 3–10 and their families. Females get head lice more often than males, and
infestation in persons of Afro-Caribbean or other black descent is rare because of hair
consistency. But, these children may have nits that hatch and the live louse
could be transferred by head contact to other children.
Head lice are spread through direct head-to-head
contact with an infested person. Body lice are spread through direct contact
with the body, clothing or other personal items or a person already carrying
lice. Pubic lice are most often spread by intimate contact with an infested
person. Head lice occur on the head hair, body lice on the clothing, and pubic
lice mainly on the hair near the groin. Human lice do not occur on pets or
other animals. Lice do not have wings and cannot jump.
From each egg or "nit" may hatch one nymph
that will grow and develop to the adult louse. Full-grown lice are about the
size of a sesame seed. Lice feed on blood once or more often each day by
piercing the skin with their tiny needle-like mouthparts. Lice cannot burrow
into the skin.
Diagnosis. In order to
diagnose infestation, the entire scalp should be combed thoroughly with a louse
comb and the teeth of the comb should be examined for the presence of living
lice after each time the comb passes through the hair. The use of a louse comb
is the most effective way to detect living lice. In cases of children with dirty, long
and/or curly/frizzy hair, an alternative method of diagnosis is examination by
parting the hair at one inch intervals to look for moving lice near the scalp.
With both methods, special attention should be paid to the area near the ears
and the nape of the neck. The examiner should examine the scalp for at least 5
minutes. The use of a magnifying glass to examine the material collected
between the teeth of the comb could prevent misdiagnosis.
The presence of nits alone however, is not an accurate
indicator of an active head louse infestation. Children with nits on their hair
have a 35-40% chance of also being infested with living lice and eggs. If lice are detected, the entire
family needs to be checked (especially children up to the age of 13 years) with
a louse comb and only those who are infested with living lice should be
treated. As long as no living lice are detected, the child should be considered
negative for head louse infestation. Accordingly, a child should be treated
with a pediculicide only when living lice are
detected on his/her hair (not because he/she has louse eggs/nits on the hair
and not because the scalp is itchy).

Louse Comb. Image Courtesy
of http://www.pediculosis-gesellschaft.de/
The most characteristic symptom of infestation is itching
on the head which normally intensifies 3 to 4 weeks after the initial
infestation. The bite reaction (Fig. 5) is very mild and it can be rarely seen
between the hairs. Bites can be seen, especially in the neck of long-haired
individuals when the hair is pushed aside. In rare cases, the itch scratch
cycle can lead to secondary infection with impetigo and pyoderma. Swelling of the local lymph nodes and fever are rare. Head lice are not known
to transmit any pathogenic microorganisms.
The most common symptom of lice infestation is
itching. Excessive scratching of the infested areas can cause sores, which may
become infected.
Head lice may cause local infections, but are not a
vector for epidemic microbial disease (see below). Head lice per se are a disease only if they cause
symptoms. In the absence of discomfort or skin lesions, infestation is
therefore only a condition and cosmetic problem for the carrier (not strictly a
disease), though they may present a disease-transmission-risk for those others
who will develop symptoms, if infected.
The number of cases of human louse infestations (or pediculosis) has increased worldwide since the
mid-1960s, reaching hundreds of millions annually. There is no product or method which
assures 100% destruction of the eggs and hatched lice after a single treatment.
However, there are a number of treatments that can be employed with varying
degrees of success. These methods include chemical treatments, natural
products, combs, shaving, hot air, and silicone-based lotions.
Treatment. Lice on the hair and body are usually treated
with medicated shampoos or cream rinses. Nit combs can be used to remove lice
and nits from the hair. Laundering clothes using high heat can eliminate body
lice. Efforts to treat should focus on the hair or body (or clothes), and not
on the home environment. Some lice have become resistant to certain (but not
all) insecticides used in commercially available anti-louse products. A
physician or pharmacist can prescribe or suggest treatments. Because empty eggs
of head lice may remain glued on the hair long after the lice have been
eliminated, treatment should be considered only when live (crawling) lice are
discovered. There are many home remedies for lice control most of that are ineffective
and some can be dangerous. The authors have a Turkish friend who had head lice
as a child and the method used on him consisted of soaking the head with
kerosene. Unfortunately, the chemical caught on fire and the individual has
been blind for virtually all his life. Other flammable materials such as
alcohol are also not advisable.
Prevention. Examination
of the child’s head at regular intervals using a louse comb allows the
diagnosis of louse infestation at an early stage. Early diagnosis makes treatment
easier and reduces the possibility of infesting others. In times and areas when
louse infestations are common, weekly examinations of children, especially
those 4–13 yrs old, carried out by their parents will aid control. Additional
examinations are necessary if the child came in contact with infested
individuals, if the child frequently scratches his/her head, or if nits
suddenly appear on the child’s hair. Keeping long hair tidy could be helpful in
the prevention of infestations with head lice. In order to prevent new
infestations, the hair of the child could be treated with 2–4 drops of
concentrated rosemary oil every day, before he/she leaves for school or
kindergarten. The oils can be combed through the hair using a regular comb or
brush. Clothes, towels, bedding,
combs and brushes, which came in contact with the infested individual, can be
disinfected either by leaving them outside for at least 3 days or by washing
them at 60°C (140 degrees F) for 30 minutes. An insecticidal treatment of the
house and furniture is not necessary.
Prevalence.
Despite
improvements in medical treatment and prevention of human diseases during the
20th century, head louse infestation remains stubbornly prevalent. In 1997, 80%
of American elementary schools reported at least one outbreak of lice. Lice infestation during that
same period was more prevalent than chicken pox.
About 6-12 million people, mainly children, are
treated annually for head lice in the United States alone. High levels of louse
infestations have also been reported from all over the world including Israel,
Denmark, Sweden, U.K., France and Australia. Normally head lice infest a new host
only by close contact between individuals, making social contacts among
children and parent child interactions more likely routes of infestation than
shared combs, brushes, towels, clothing, beds or closets. Head-to-head contact
is by far the most common route of lice transmission. The number of children
per family, the sharing of beds and closets, hair washing habits, local customs
and social contacts, healthcare in a particular area (e.g. school) and socio
economic status were found to be significant factors in head louse infestation
. Girls are 2-4 times more frequently infested than boys. Children between 4
and 13 years of age are the most frequently infested group.
The United Kingdom's National Health Service, and many
American health agencies, report that lice "prefer" clean hair,
because it's easier to attach eggs and to cling to the strands, however, this
is often contested.
Because head louse infestation occurs primarily in
children, much of the effort to
prevent head lice transmission has focused on school and day care
settings—places where large numbers of children come into close contact.
Schools in the United States, Canada, and Australia commonly exclude infested students, and prevent return of those
students until all lice, eggs, and nits are removed. This is the basis of the "no-nit
policy". Data from a primarily American study during 1998-1999 found that
no-nit policies were present at 82% of the schools attended by children
suspected of louse infestation. A
separate 1998 survey revealed that 60% of American school nurses felt that "forced absenteeism of any
child who has any nits in their hair is a good idea.
School Head Lice Policy. This involves a number of issues:
Establishing criteria to infer infestation; screening asymptomatic
children for evidence of infestation; establishing the
circumstances under which children will be inspected; immediate exclusion of
infested children; and establishing criteria to permit previously infested
children to return to school (e.g., the no-nit policy).
All of these policies are controversial.
In particular, a number of health researchers and organizations object to the
required removal of nits (i.e., the no-nit policy). Opponents to the no-nit policy point
out that nits, being empty egg casings, have no clinical importance. Transmission can only occur via live
lice or eggs. Time-consuming nit removal, therefore, has no direct effect on
transmission. This has led to the perception that the no-nit policy serves only
to ease the workload of school nurses and punish the parents of infested
children.
Proponents of the no-nit policy counter
that only a consistently nit-free child can be reliably shown to be
infestation-free. That is, the
presence of nits serves as an indirect proxy for infestation status. Proponents
argue that such a proxy is necessary because lice screening is prone false
negative conclusions (i.e., failure to find lice present on actively infested
children).For example, a 1998 Israeli study found that 76% of live lice
infestations were missed by visual inspection (as verified by subsequent
combing methods). Although lice
cannot fly or jump, they are fast and agile in their native environment (i.e.,
clinging to hairs near the warmth of the scalp), and will try to avoid the light used
during inspection. Lice colonies
are also sparse (often fewer than 10 lice), which can contribute to difficulty
in finding live specimens. Further,
lice populations consist predominantly of immature nymphs, which are even
smaller and harder to detect than adult lice.
Body Lice. The
behavior of body lice, which are also called cooties, is totally different than
that of head lice. Females lay up to 300 eggs and the life cycle can be
completed in as little as 25 days. The eggs are deposited on clothing and the
nymphs and adults remain on clothing, even while feeding. Body lice
infestations are not common in California, but typically develop when a large
number of people live closely together under poor sanitary conditions, such as
during war time. One person can harbor a large colony of this species. Over
30,000 body lice have been removed from a single individual. Even though such
an infestation is rare, these insects have such a rapid reproductive capacity
that huge numbers can develop rapidly unless control is quickly initiated. Close
contact with someone who is heavily infested can result in a transfer of
several hundred lice to a non-infested individual.
As in the other two species that attack humans, body
lice cause dermatitis and considerable irritation. Scratching can result in
secondary infection and sometimes blood poisoning. In long term infestations a
condition called vagabond’s disease may develop. The victim’s skin becomes
thickened and deeply pigmented. This condition is not due to a microorganism,
but to the skin’s reaction to the feeding of the lice. Finally, individuals who
are heavily infested with lice may develop a systemic or overall body, effect.
The following is taken from a report made by a scientist who recorded his
symptoms after allowing 700 to 800 lice to feed on him two times a day. "I
started feeding twice a day and almost immediately a general tired feeling was
noticed in the calf of my legs and along the shin bones, while on the soles of
my feet and underneath my toes the tired feeling was so intense as to often
prevent sleep until late in the night. An irritable and pessimistic state of
mind developed. An illness resulted with symptoms very similar to grippe and a
rash similar to German measles was present, particularly over the shoulders and
abdomen." Once the experiment was discontinued the symptoms disappeared
within a few days.
Body lice are capable of vectoring diseases; the most
important of which is epidemic typhus. Based on actual human deaths, this is
one of the top three insect-vectored diseases in the world. The etiological
agent is Rickettsia prowazeki and the primary vector is the body louse.
Body lice are the main transmitters, perhaps because head lice are less mobile
and they don’t reach the high populations on the body—therefore they are less
frequently passed from person to person. Epidemics usually occur in the winter
when people are huddled closely together and the lice migrate nightly from one
pile of clothing to the next.
The rickettsias multiply in the epithelial cells of
the louse intestine and are voided with the feces. After feeding, body lice
defecate next to the bite; subsequently, the rickettsia can be scratched into
the bite by the host, thus establishing the disease. After a period of time the
feces dries and the rickettsia become airborne resulting in transmission
through inhalation.
Historically, this disease has been instrumental in
the outcome of several wars. In some cases, it has killed more soldiers than
fighting. Epidemic typhus was a major factor in Napoleon's withdrawal from
Russia. During World War I this disease killed over 3 million Russians. Typhus
was again threatening in the early years of World War II. During 1942 there
were 83,000 cases in North Africa. When allied forces landed in Italy in l943,
a typhus epidemic was well underway in Naples, a city of about 1 million
people. There was congestion, unsanitary conditions, food scarcity and
malnutrition. The death rate was around 81% and it was quite likely that the
entire city would have been annihilated, if not for a very effective louse
control program initiated by the allies. The program consisted of applying 10%
DDT dust to the clothing of the majority of the city’s inhabitants. The people
were lined up for blocks. The DDT was applied from a backpack duster with an
attached elongated tube. The tube was inserted into the shirt and/or pants of
the individual to be treated and then the duster was turned on—as a result he
dust was blown throughout the clothing.
Epidemic typhus is characterized by severe headache,
high fever and a rash caused by small hemorrhages. Today the disease is kept in
check by vaccines, modern antibiotics, and the use of pesticides to prevent the
buildup of louse populations.