CHAPTER 5

Arachnids-Ticks
and Mites
This
is the second largest order (insects are first!) of plants and animals. Most
experts believe there are over one million species of these arachnids that
occupy nearly every ecological niche. For example, almost anyone reading this
CD is currently infested with mites. There is a small mite that lives in hair
follicles and the sebaceous glands of the nose. They are harmless and should be
of little concern. There are even mites that live in the lung cavity of the common
garden snail and, unlike insects mites occupy many areas of the ocean.
The
mites and ticks are separated from other arachnids by the sac-like body. The
abdomen is not distinctly segmented, but rather, is joined broadly to the
cephalothorax. The mouthparts of these small animals are primarily for piercing
a host and then sucking up juices.
Mites
generally are quite small (most are smaller than a grain of sand). Some are
microscopic. Because of the large number of species in this group, almost every
conceivable feeding habit is exhibited. Mites are not only found in almost
every ecological habitat, but they are one of the most common creatures on
earth.
The
basic life cycle of mites and ticks is: egg, larva, nymph and adult, with the
larval and nymphal stages looking like smaller versions of the adult; however,
the larvae bear only six legs each while the adults bear eight.
ENTOMOPHOBIA
These
two distinct phenomena are both based on the fear of small creepy creatures. As
the name implies, entomophobia is the fear of insects. Based on a national
survey, the fear of insects is ranked third in adults—closely behind the fear
of public speaking and death. The fear of cockroaches is frequently ranked
number one in the insect world. Possibly
the fear of insects is a learned response. Very few children are afraid of
insects unless they learn to be so by their parents, movies, or other sources.
Because this is a learned response, this type of fear frequently can be
reversed—sometimes with very little effort.
We
have found that exposure to reptiles and insects is often enough to
"unlearn" this fear. Once a young person can be persuaded to hold a
walking stick and then to look into its "cute little face," they are
halfway to undoing an acquired fear of all six legged animals. We have observed
this behavior time and again due to our activity with youth fairs and other
such public events. The annual county fair in
We
once participated in a youth exposition where management sent us a teenaged
girl to help out. Being deathly afraid of snakes, she probably was not the best
volunteer for our type of exhibit! She assured us she would be all right as
long as she didn’t have to go near anything reptilian. After a short period of
time, she ventured a small caress down the back of our most beautiful snake.
Then she had us hold its head so she could feel what the body felt like. Then
she bravely held the whole snake. The snake, responding to a warm body in a
cold room, coiled delicately around her arm and cuddled right up. By the end of
the day, she wanted to take it home with her. For most people, this intimacy
experienced with the previously feared insect or snake is enough to overcome
many years (sometimes decades) of learned terror.
Delusory
parasitosis is a paranoia, or irrational fear, of small creepy non-existent
creatures. Because mites are so small, in many cases this condition is
diagnosed as a mite infestation. This phenomenon is more common than one might
expect. Frequently, people who are inflicted with this malady are quite normal
in all other phases of life and lead productive lives.
I
was quite unaware of this phenomenon until one day a man in his mid 40's walked
into my office and indicated that the
There
have been many similar situations since then. One of the most unusual occurred
a few years ago when a city official from Mission Viejo (Orange County) called
me and indicated that he had a whole neighborhood infested with scabies mites
(see below). Scabies are parasitic mites that commonly infest humans. At the
time this didn’t seem questionable because a number of the people had been to
medical doctors and had been treated for this mite. These treatments didn’t
seem to solve the problem, so I was brought in as a consultant. The main
problem was centered on one particular resident. This woman apparently had
convinced much of the neighborhood of the widespread infestation. She was using
very drastic measures to try to eliminate these mites from her house and
family. She would use lye to scrub down the beds on a weekly basis. On several
occasions she washed her kids down with gasoline. Of course, upon hearing this,
I began to realize that the whole situation was more than a little irrational.
The final clincher was when she indicated that the whole problem started when
she brought a potted plant back from Arizona and, while it was sitting in her
bathroom, a pod grew out of it and blew these tiny critters all over the
neighborhood.
A
colleague from NCSU, Mike Waldvogel, reports similar experiences. He states he
has received a variety of imaginary critters in vacuum cleaner bags, pillows
cases, panty hose, skin samples, glue boards (like the one you use for catching
mice) and (the one he described as the ultimate) a bottle (formerly a pint gin
bottle) that was labeled "after douching." Needless to say that one
wasn’t opened! Neither were the vacuum cleaner bags, as they usually contain
pesticide-laden dust from over treated carpets for these so called pests.
All
of these cases have had several symptoms in common. The 'critters' typically
fly through the air, crawl on the skin, frequently appear and disappear in the
skin, make clicking noises and can be found in soap and toothpaste. Generally,
inflicted individuals have gone to several medical doctors to no avail and can
almost never be persuaded that the pests are imaginary.
Scabies of Mange Mites. Sarcoptes scabei is a parasitic mite that
attacks a wide variety of mammals; however, there are many varieties, with each
type being host-specific. For example, the variety of scabies that attacks
humans does not infest other animals.
Similarly the scabies mites that attack dogs do no infest humans. The human scabies mite is almost invisible to
the naked eye (about 1/60 inch), cylindrical in shape, and has golf tee-shaped
suckers on the tips of the legs (Figure 5A).
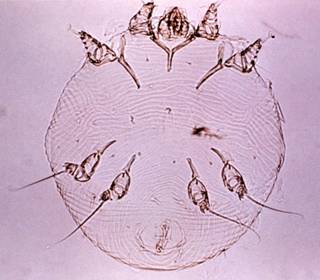
Figure 5A. A female human sarcoptic
mange mite (Sarcoptes scabei) greatly magnified. Image courtesy of CDC Healthwise Photo Library.
The
life cycles of male and female human scabies mites are somewhat different. A
young female adult will crawl over the human body until she reaches soft
wrinkly skin and, within two to three minutes, bores inward, forming a tunnel
about 3/4" in length and parallel to the skin surface. She feeds on body
juices and lays eggs (up to 20 per female) in the burrows. With close
inspection mature females can be seen in the burrows. As a result of this activity, pimple-like
structures develop which eventually rupture after a day or two, releasing the
eggs on the skin. Once hatched, the larval and nymphal stages crawl over the
skin and periodically feed in sebaceous glands and hair follicles. Male mites
also feed in these areas. Generally it takes about two weeks to complete the
life cycle from egg to adult.
Scabies is nearly always acquired by skin-to-skin
contact with an infested individual. The contact may be quite brief such as
holding hands. Frequently it is acquired from children, and sometimes it is
sexually transmitted. Occasionally scabies is acquired via bedding or
furnishings, as the mite can survive for a few days off its human host.
The
majority of the mites (63%) are found on the hands (especially between the
fingers) and wrists (Figure 5B) and about 11% on the elbows. In women the mites
are often found burrowing beneath and around the breasts and nipples. In young
children, whose skin is still soft, the mites can be found all over the body
and frequently on the legs.

Figure 5B. Scabies infestation between fingers. Image courtesy of CDC Healthwise Photo
Library.
There are no obvious symptoms for the
first 30 days after infestation. During that period, treatments are not
necessary. However, subsequently, an intense rash and itching begins to occur
over many areas of the body, in some cases even in areas where the mites are
not found. The itch is characteristically more severe at night and affects the
trunk and limbs. It does not usually affect the scalp. Itching can become so
intense that the infested person loses sleep and can be affected mentally.
Blisters and pustules on the palms and soles are characteristic of scabies in
infants. Secondary infection commonly
complicates scabies and results in crusting patches and scratched pustules. After about 100 days the mite population
drops off and symptoms of the infestation begin to disappear.
Treatment
consists of elimination of the mites from the body and treatment of recently
worn clothing and bedding. The mites are totally host dependent and can not
live off the host for more than a day or two. Pesticide lotions can be used to
kill those mites on the body. Kwell
lotion was the standard for control for many years. However due to possible negative side effects
of the active ingredient, it has been mostly replaced with more effective products.
Recently used clothing or bedding should be laundered, ironed or sealed in
large plastic bags for a few days. Symptoms will not disappear completely for a
few weeks after the mites are eliminated.
This is significant because it is probably not a good idea to over-treat
an infestation of these mites. One of our
grandkids contacted scabies and the kids next door had the same problem. We instructed the neighbor how to treat her
kids. About a week later she indicated
that the symptoms had not disappeared and wanted to retreat her kid. This is not a good idea as exposing children too
frequently to the prescribed pesticide can lead to overmedicating. Therefore it’s important to know and to
follow the directions for such direct contact treatments.
It
should be mentioned that medical doctors frequently misdiagnose scabies mite
infestations. As discussed above, several of the neighbors of the lady
suffering from delusory parasitosis were convinced by her that they had scabies
and were actually diagnosed and treated for them. I was once suffering from
itching of the skin and went to a M. D. who immediately, upon hearing my
symptom, stated that I had scabies and prescribed Kwell. I told him that I
really didn’t have any of the other symptoms other than itching. His response
was "sometimes there are no other symptoms," which may or may not be
true. The point is that he didn’t even look at me. Upon hearing
"itching" he stepped back about two feet (they are fairly contagious)
and muttered "scabies.” After using the Kwell with no relief, I consulted
a dermatologist who correctly diagnosed my problem as dry skin.
I
was recently contacted by a convalescent home about a scabies infestation. They had approximately 100 patients half of
which were diagnosed with scabies. This
was a real problem. Public Health had
quarantined the hospital because this is a communicable disease. Of course this was devastating and confusing
to the older residents as their relatives couldn’t visit them. The people who worked there were very
concerned and fearful that they might carry the disease home with them and give
it to their own families. With this in
mind, the hospital wanted me to come up with a viable treatment program. Treatment was several fold. Everyone involved had to be treated with
Kwell lotion-the chemical that at that time was preferred. Treatment included all the patients and
individuals who worked there as symptoms of an active infestation do not appear
immediately. There was no need to treat the premises itself as the mites are
host-dependent and can only live off the host for a day or two. However, recently worn clothing and bedding
had to be treated as a potential source of infestation. We considered sending these to a commercial
laundry, but that created the potential of infesting the individuals who worked
there. Instead, we took all the clothing
and bed sheets and sealed them in large trash bags for three days, keeping in
mind that the mites can only survive off the host for a day or two.
House
Dust Mites. These are not visible to the naked eye
and are not typically found, as is implied by the name, in house dust (Figure
5C). These arachnids feed on
human dander (sloughed skin) and thus are found in areas of the home where this
material accumulates, such as in beds or sofas. They tend to be more common in
humid areas and where cotton is used as stuffing in furniture. House dust mites
do not bite, but have been implicated in certain types of allergies in humans.
These arachnids at one time or another infest most homes in many parts of the
country.

Figure 5C. A common house dust mite
greatly magnified.
Image
courtesy of ARS.
These tiny arthropods should not be of any concern to
the average homeowner. They do no bite
and their presence is generally undetected due to their microscopic size. However their presence can cause one
problem. Some individuals become
allergic to the tiny specks of protein in the form of the house dust mite
itself. Allergic symptoms include runny
nose, red eyes and sneezing.
One major mattress companies has an advertisement on
TV that states that the weight of an average mattress in the US doubles in 10
years as it fill up with house dust mites.
They also claim that their mattresses are built so well that these mites
cannot get inside them. Of course both of
these statements are ridiculous. First
of all house dust mites do not get inside mattresses and if they wanted to I
doubt that they would have any problem considering their size. Secondly a queen size mattress weighs around
60 pounds. Sixty pounds of house dust mites would be in the billions and there
is no way there would be enough food (dead skin) to support a population of
that size.
.
Chiggers.
This is a group of mites that are parasitic on humans, snakes, turtles,
rabbits, chickens, and many other animals. Adults and nymphal chiggers are typically
free-ranging (Figure 5D) scavengers associated with the soil and commonly are
found in meadows, grasslands and wooded areas. Chiggers are present in Southern
California, but are much more common in the southeastern United States and many
tropical areas of the world.

Figure 5D. An adult chigger. Image
courtesy Susan Ellis, Bugwood.
An excellent example showing how common chiggers and
other arthropods can become was documented a number of years ago in the Arizona
desert. An entomologist from the
University of Kansas was flying over the Arizona desert at an elevation of
around 1,500 feet when he spotted a reddish bloom covering approximately two
acres. Upon landing he was amazed that
it was a heavy emergence of giant red velvet mites. Keeping in mind that these mites are “giant,”
but no larger than the size of a 0 on this page, the estimated population was
approximately three to five million with an average of 50 mites per four inch
square.
Their
eggs are deposited in clusters in the soil. Upon hatching, the parasitic larval
stage will accumulate on vegetation, stones or other objects to await a passing
host. Chiggers and other ectoparasites recognize a host by 3 means: mainly the
host’s movement, heat and odor in the form of carbon dioxide.
Chiggers larvae are tiny-less than 1/150th
of an inch in diameter. More than a thousand of them could line up across this
page and still leave room for two or three hundred more. At this size, chiggers
are almost invisible to the unaided eye. However, when several chiggers cluster
together near an elastic waistband or wristwatch they can be seen because of
their bright red color.
One of the greatest misconceptions about chiggers is
that they burrow into our skin and eventually die within the tissues, thus
causing the persistent itch. Chiggers attach by inserting minute specialized
mouth parts into skin depressions, usually at skin pores or hair follicles. The
chigger's piercing mouth parts are short and delicate, and can penetrate only
thin skin or where the skin wrinkles and folds. Chiggers typically bite around
the ankles, the back of the knees, about the crotch, under the belt line and in
the armpits, mainly because these are areas of the body where the skin is soft.
The insertion of the mouth parts is not perceptible. The bite alone is not the
source of the itch.
A feeding chigger usually goes unnoticed for one to
three hours after it starts feeding. During this period the chigger quietly injects
powerful digestive saliva. After a few hours your skin reacts by hardening the
cells on all sides of the saliva path, eventually forming a hard tube-like
structure called a stylostome.
The stylostome walls off the corrosive saliva, but it
also functions like a feeding tube for the hungry chigger. The chigger sits
with its mouthparts attached to the stylostome, and like a person drinking a
milk shake through a straw; it sucks up your liquefied tissue. Left
undisturbed, the chigger continues alternately injecting saliva into the bite
and sucking up liquid body tissue.
It is the stylostome that irritates and inflames the
surrounding tissue and causes the characteristic red welt and intense itch. The
longer the chigger feeds, the deeper the stylostome grows, and the larger the
welt will eventually become. The idea that the welt swells and eventually
engulfs the feeding chiggers is also a myth. Many people have seen a small red
dot inside a welt (usually under a water blister), but this is the stylostome
tube and not a chigger body.
The time required for a chigger to complete its meal
varies with the location of the bite, the host and the species. If undisturbed,
chiggers commonly take three or four days, and sometimes longer, to eat their
dinner. This is not surprising when you consider that this is the first and
last meal of the young chigger's life. On human hosts, however, chiggers seldom
get the chance to finish a meal. The unlucky chigger that depends on a human
for its once-in-a-lifetime dinner is almost sure to be accidentally brushed
away or scratched off by the victim long before the meal is complete.
The intense itching usually peaks a day or two after
the bite occurs. This happens because the stylostome remains imbedded in the
skin tissue long after the chigger is gone. The skin continues the itch, an allergic
reaction to stylostome for many days. The stylostome is eventually absorbed by
the body, a slow process that takes a week to 10 days, or longer.
Women and children get more bites than men. Folklore
says that if chiggers have a choice, they will attack women before men. But the
truth is that men, women and children collect the same number of chiggers
during a walk in the woods. Women and children generally have thinner skin, and
thus more surface area that chiggers can easily bite.
The first line of defense against chiggers is the
right kind of clothing. Shorts, sleeveless shirts and sandals are nearly
suicidal in chigger-infested areas. Wear tightly woven socks and clothes, long
pants long sleeved shirts, and high shoes or boots. Tucking pant legs inside
boots and buttoning cuffs and collars as tightly as possible also helps keep
the wandering chiggers on the outside of your clothes.
Regular mosquito repellents will repel chiggers. All
brands are equally effective. Applying these products to exposed skin and
around the edge of openings in your clothes, such as cuffs, waistbands, shirt
fronts and boot tops, will force chiggers to cross the treated line get inside
your clothes. Unfortunately these repellents are only potent for two to three
hours and must be reapplied frequently.
People
who live in chigger-infested areas may develop immunity to the bite of these
arachnids. Humans who have been exposed to chigger bites over a period of years
may develop a hypersensitivity to their saliva. Hence, when they are newly
bitten, a huge tissue hardening occurs (rather than the feeding tube) almost
immediately that actually prevents further penetration of the skin; thus,
little saliva is injected and no further symptoms may occur
Ear
Mites. This is a group of parasitic mites that attack a variety of animals, including cats,
dogs and rabbits. In these animals, infestations are limited to the ears and
the mites are typically found feeding in the outer ear canals. As do most
parasitic arthropods, ear mites are host-specific and no species attack humans.
In rabbits, infestations can become serious if left uncontrolled; the result
can be bleeding, secondary infection and possible death. An infestation is
easily recognized by a layer of dried ooze on the inner side of the ear. If
this crusty ooze is removed, large numbers of mites can be found feeding on ear
tissue.
As
discussed, ear mites are common in dogs and cats. Young animals appear to be
more susceptible to the feeding of these arachnids. Typical symptoms include
frequent shaking of the head, lowered ears (in cats), and nearly black
coloration in the outer ear canal (this gives the appearance that the animal
has very dirty ears).
In all cases
a few applications of several drops of mineral oil to the infested area will
give considerable relief and control, although most veterinarians suggest this
should be followed by applications of medications specifically used for ear
mite control. It should also be noted that bacterial and fungal infections of
the ears result in similar symptoms.
Human Follicle Mites. Follicle mites are long and skinny with short legs
(Figure 5E). These microscopic mites infect many species of mammals, and
they seem to have a high degree of host specificity (i.e., mites from one host
species will not infect another host species).
Humans are infected with Demodex folliculorum, which lives in
hair follicles and sebaceous (oil) glands, especially around the face
(particularly in and around the nose, eyes, and forehead). This mite occurs in a high percentage of the
population (nearly 100% in older people), but, fortunately, it normally does
not cause "problems." In those
cases in where follicle mites do cause problems, they are most often associated
with skin rashes, hair loss (particularly the eyelashes), and acne.
In other animals, infections with follicle mites can
be more serious. Dogs are infected with D.
canis (the dog follicle mite) which can cause red or canine demodectic
mange. This mite can cause severe skin
problems in infected dogs, including significant loss of hair and skin
rashes. In severe cases infected dogs
may be euthanized.

Figure 5E. A human follicle mite. Image courtesy of Life
Science Dept., University of South Africa.
Phytophagus
Mites. These are a large group of mites that are plant feeders
(phytophagous). The most common type of these is spider mites that typically
feed on the undersides of leaves by puncturing the plant surface with their
mouthparts and sucking plant juices. These are not only a major pest of many
agricultural crops but also attack most types of houseplants.
The
most obvious symptom of feeding by spider mites in the early stages of an
infestation is a fine speckling that appears on the upper surface of the leaf
(Figure 5F). As the infestation advances, fine webbing results. Generally, by
that point, the plant is beyond saving.


Figure 5F. A cotton leaf with typical
spotting due to feeding of phytophagus mites. Right image greatly magnified
spider or two spotted mite-actual size about the size of the period at the end
of this sentence. Image courtesy of ARS.
The
main predators of spider mites are other mite species. It is therefore
important to be able to distinguish predatory mites from phytophagous forms.
Again, as with other arthropod groups, predators are quite fast while plant
feeding forms move slowly or are nearly stationary. A good rule of thumb is if
you can see it moving it’s a predatory mite. Plant feeding mites are best
controlled with pesticide, in this case, an acaracide. Some degree of control
may be achieved by periodically washing the mites off the plant with a mild
soapy water solution.
Ticks. Ticks are of considerable economic
importance, as they suck blood and vector a number of diseases to humans and
other animals. These arachnids may be distinguished from mites by their large
size and leathery exoskeleton (Figure 5G).

Figure 5G. A typical hard tick prior to
feeding.
There
are two families of tick: namely, the hard and soft ticks. The soft ticks
almost exclusively attack birds and are of minimal concern to the general
public. Hard ticks, as do all Acari, pass through four developmental stages.
The eggs of most hard ticks are deposited in clusters in protected locations
such as in the soil; there may be as many as 7000 eggs in a single cluster
(Figure 5G). Upon hatching, the six-legged larvae (seed ticks) crawl up on
vegetation and wait for a passing host. Once attached to a host, they burrow
their heads below the skin and begin to suck blood. Hard ticks feed to
engorgement, swelling with blood to many times their original size (Figure 5H).
They feed continuously for a day or more before dropping to the soil and
eventually molting into the eight-legged nymph. The nymphal and adult stages
repeat the process of waiting for a host and feeding to engorgement.

Figure 5H. A hard tick fully engorged
with the blood of its hosts.
Image courtesy of Charles Lewallen.
The
length of development from egg to adult depends primarily on the availability
of food and takes place anywhere from a few months to longer than a year. The
larval or nymphal stages may have to wait for up to several months for a
passing host. Apparently this has little effect on survival, as these stages
generally can live 300 or more days without feeding.
Most
ticks require three separate hosts to complete their life cycle and are
referred to (surprise!) as three-host ticks. A few species will remain on or
near the same host during the larval and nymphal stages, but go to another host
during the adult stage and are referred to as two-host ticks. One-host ticks
spend all three stages on the same host.
The brown
dog tick is probably the most widely distributed
species, not only in the United States, but also in the entire world. It is
found in both tropical and temperate climates. It is a three-host tick that, as
its name implies, prefers dogs; however, it occasionally feeds on other animals
such as cattle, horses and (occasionally) humans. This species is unique, in
that it prefers to live and breed in protected locations such as homes and
kennels. It is not uncommon to encounter large infestations in homes.
The
authors encountered a huge infestation of this tick in a one-bedroom apartment;
the owner had gone on vacation and left a German shepherd in a kennel.
Apparently prior to this an impregnated female tick attached itself to the dog
and was brought home. The tick dropped off and deposited from 2000 to 3000 eggs
in the house. Because the ticks had a continuous source of food (the dog) and a
favorable environment, development was fast. Over 400 ticks were vacuumed from
the apartment. Because the preferred host was present, none of the residents
were bitten. However, ticks commonly were found crawling around the apartment
and frequently were squashed accidentally, leaving blood spots on the furniture
and beige rug.
The
wood
tick is another three-host species that commonly
occurs in the forests and scrubland of California and other western states. It
readily attacks humans and is a primary vector of Rocky Mountain spotted fever.
The disease is occasionally found in the Rocky Mountain States but normally
does not occur in California. In addition, in the Rocky Mountains states, the
feeding of female wood ticks around the cranial areas can result in tick
paralysis in humans and other animals. This paralytic condition apparently
occurs due to the injection of saliva. It can be fatal, but, if the tick is
removed, recovery is complete.
If
a tick is pulled off the host’s body while it is feeding, its mouthparts may be
left in the wound and a secondary infection or blood poisoning could result.
The basic premise behind proper removal is to provoke the tick to withdraw its
mouthparts. It was once thought that touching a hot match or needle to the back
of the abdomen was an effective means of tick removal. This technique is no
longer recommended as it may cause the tick to regurgitate, which can transmit
disease-causing organisms. Today, coating the tick for a short time in Vaseline
or careful removal with forceps are the recommended methods.
LYME DISEASE
This
disease was first diagnosed in 1969 in the United States in Old Lyme,
Connecticut. It now occurs in 43 states. Nationwide it has quickly increased
from 2,300 human cases in 1986 to 7,400 in 1989. Since then the number of cases
in the United States has increased steadily, with a whopping increase of 40% in
1997. New York State had over 5000 cases in 1997. Lyme disease has not been
found in Southern California, but is prevalent in Northern California and in
the eastern United States. In California the western black legged-deer tick is
the primary vector of this disease.
The
symptoms of Lyme disease are several fold. A rash generally develops from 3 to
30 days after the initial bite. Shortly after, large donut-shaped blotches (Figure
5I) develop (not necessarily at the site of the bite). Within weeks to months
after these initial symptoms, a number of chronic conditions may
occur—including facial paralysis, malfunction of arms and legs, heart
abnormalities, migratory pain in the joints, arthritis and deterioration of the
bones.

Figure 5 I.
Typical early symptom of Lymes disease-donut shaped rash. Image courtesy of CDC Healthwise Photo
Library
This
disease rarely results in death; but, if allowed to advance, can be
debilitating indefinitely. It is important to be able to diagnose this disease
during the initial symptoms, as it can be treated successfully with
antibiotics. Treatment is much less successful in the advanced stages. In
states where this disease is prevalent, it is best to apply repellents (OFF)
around the ankles and pant cuffs while in those areas where ticks are found.
The authors know several individuals from Southern California who have
contracted the disease. In their cases the disease was contracted in the
Eastern U.S. or in Northern California. An important factor is that, when they
came back to Southern California, their doctors had a rather difficult time
diagnosing the disease as they had not seen very many cases.